Few people living today remember what it was like to live through a world war, but that’s what we’re in, and we’re going to have to sacrifice if we want to save ourselves and each other. Just as the greatest generation did, we need to step up to what history has delivered.

The United States has the highest coronavirus death toll in the world.
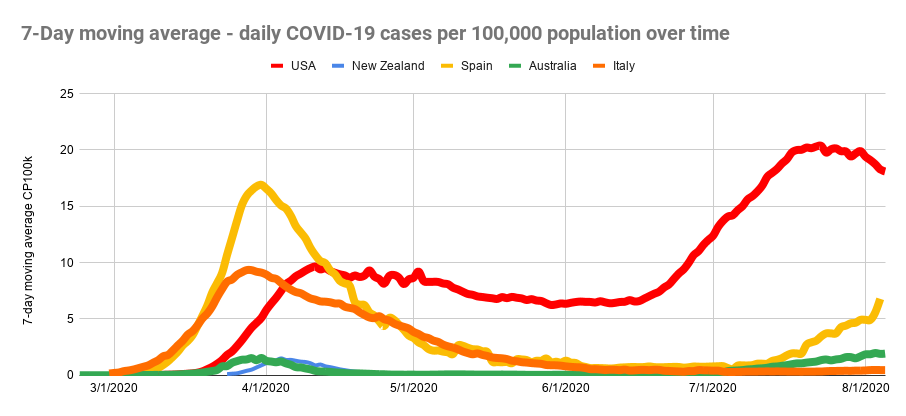
It didn’t have to be this way — and in most developed countries, it isn’t. Countries like Germany, Singapore, Australia and Japan have fractions of our death rate.
If our response had been as effective as Germany’s, we would have had 36,000 COVID-19 deaths by mid-June in the United States, instead of 117,000. If our response had been as effective as South Korea, Australia or Singapore’s, fewer than 2,000 Americans would have died by then. We could have prevented 99% of those COVID-19 deaths. But we didn’t. And today, the number of coronavirus-related American deaths has passed 170,000.
How did this happen?
In the spring, we shut down our lives and our economy in hopes of reducing the spread of COVID-19 enough to be able to manage it through widespread testing and contact tracing. In spite of that shutdown, today the virus is raging virtually uncontrolled. California recently declared defeat on the whole concept of contact tracing, because there are too many cases to trace. Other states are quite obviously in the same situation.
Was shutting down the wrong approach?
Clearly not. It worked in other countries. So what went wrong here?
We didn’t stick with it until the job was done.
Given our current situation, a shutdown that succeeds in suppressing the spread of the coronavirus is both the best way to save lives and the fastest way to start moving safely back toward social life.
But a shutdown is only effective if it lasts long enough and is comprehensive enough to interrupt transmission of the virus. An effective shutdown reduces the total number of infected people to the point where cases are rare enough to monitor and contain. Then, robust testing and contact tracing are critical to containing isolated outbreaks before they explode.
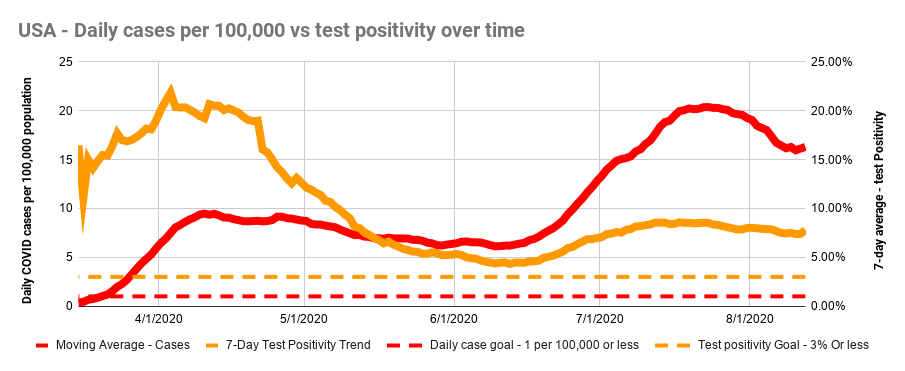
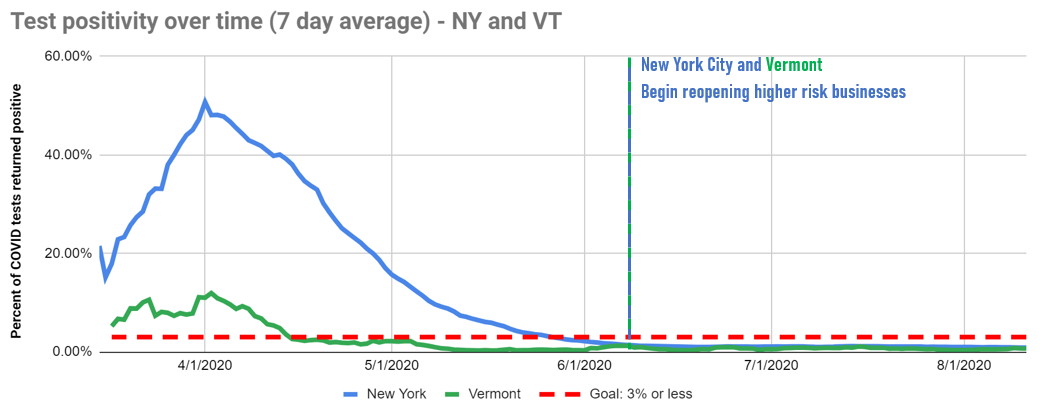
Public health experts have identified two key indicators for when it’s safe to lift a shutdown:
The rate of new daily cases should be less than 1 per 100,000 people in the population.
Less than 3% of people tested should have a “positive” test result. At that level, we can effectively trace new cases and contain new outbreaks.
That second indicator assumes that we are doing a lot of testing — enough to get a true picture of what is going on. Harvard’s Global Health Institute has said that to squelch the virus, we’d need to process about 4.3 million tests per day — which unfortunately is a staggering goal due to federal inaction to increase our capacity to create, ship, administer and evaluate COVID tests.
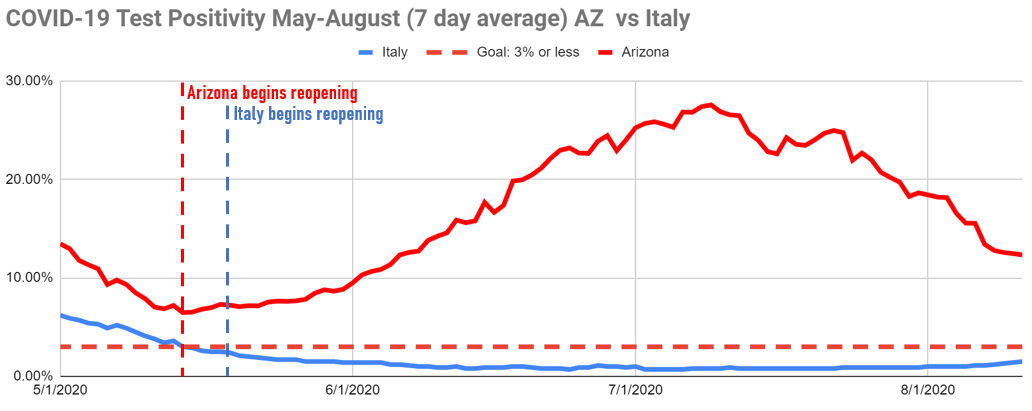
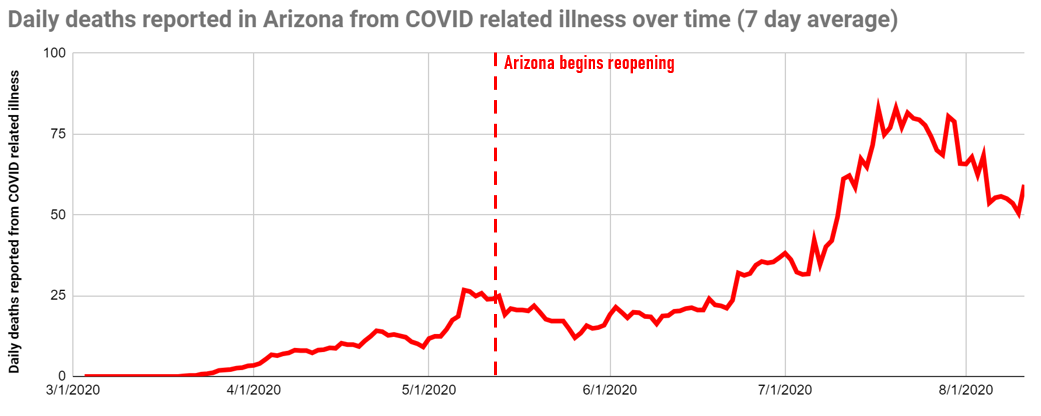
Using those key indicators, let’s look at what has happened in Arizona. COVID-19 case growth was slow in our state until May, when the state began lifting restrictions on high-risk businesses on the 11th.[i] The effects of reopening became clear three weeks later, as case growth exploded, eventually reaching 53 per 100,000 per day.[ii] That’s 52 times higher than the target.
Our daily average cases peaked more than five times higher than the daily average case rate in Italy in mid-March, when that country was the epicenter of the outbreak in Europe.
In contrast, Italy’s emergence from shutdown, which started shortly after ours, was much more successful. Adherence to the guidelines for daily cases and positivity rates resulted in a far better outcome.
These charts tell the story:
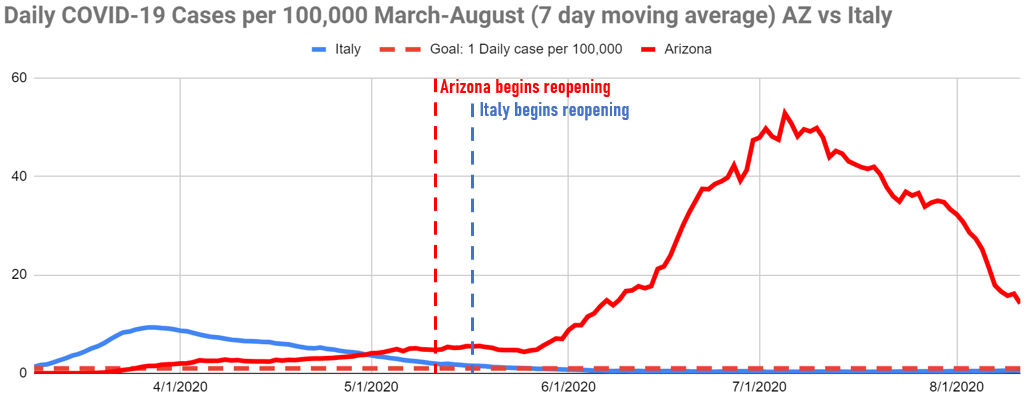
Data from Our World in Data COVID-19 Dataset.
Former Director, Public Health Campaigns, PIRG